|
��Deep Brain Stimulation: DBS
At our Center, we have been performing Deep Brain Stimulation (DBS) since May 2010. We were the first hospital in Shiga Prefecture to offer this procedure to our patients. DBS is performed using the Leksell stereotactic apparatus. This is the same apparatus used in Gamma Knife surgery, and therefore the treatment plan is also similar. We have performed over 1,000 procedures using this apparatus.
1.What is Deep Brain Stimulation?
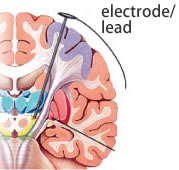
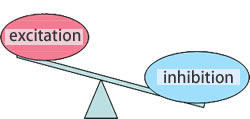
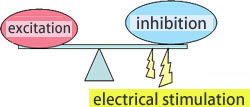
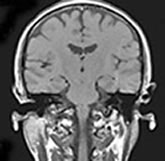
Using stereotactic surgery, an electrode (also called the lead) is placed into the deep region of the brain (figure 1), and the electricity sent through the electrode reduces excessive suppression, rebalances neuronal excitation, and helps to improve symptoms (figure 2).
It should be noted that this procedure helps improve the symptoms, but is not a curative treatment of the disease.
 |
| Figure 1 |
Figure 2 |
 |
| �yBefore the stimulation�z |
 |
| �yAfter the stimulation�z |
 |
�Q.Candidates for DBS Treatment
DBS is suitable when symptoms cannot be controlled with medication or when the patient cannot tolerate the side effects of the medication and its use is no longer appropriate, and when the potential effectiveness of the stimulation appears promising.
�R.How is DBS Performed?
| �@The frame is attached |
|
�AMRI Scan |
 |
 |
 |
|
|
 |
|
|
�BThe target is set |
 |
 |
 |
|
|
|
| �CThe electrode is inserted and microelectrode recording is done |
 |
|
|
|
| �DThe electrode is placed |
|
�EThe pulse generator is implanted |
 |
|
 |
|
�S.Postoperative Management - Adjusting the Stimulation
As the patient�fs medication is gradually reduced,the stimulation parameter is reprogrammed each time the medication is adjusted.
|
 |
The various stimulation settings can be adjusted through the skin. The optimal setting will be determined after the surgery. |
|
 |
��The patient turns the pulse generator ON/OFF. |
|
�T.Complications/Side-Effects of the Treatment
- �yComplications related to surgery�z
�@�@�@��Intracerebral hemorrhage, infection, etc.
- �ySide-effects of the stimulation�z
�@�@�@��Temporary psychoneurosis such as hallucinations
�@�@�@�@�@Dyskinesia (temporary), etc.
- �yEquipment related issues�z
�@�@�@��Infection, malfunction such as wire disconnecting, etc.
��Parkinson�fs Disease
1.Causes of Symptom�@Manifestation
The part (tonsil) of the cerebellum descends causing the obstruction of the flow of the spinal fluid, which causes the fluid to be retained in the spinal cord creating a cavity. The symptoms tend to include neurotrophic pain on the hands and in the lateral region of the abdomen, deformed joints, scoliosis, and muscle atrophy in the hands. It is often possible to slow the progression of the disease by a procedure called Foramen Magnum Decompression.
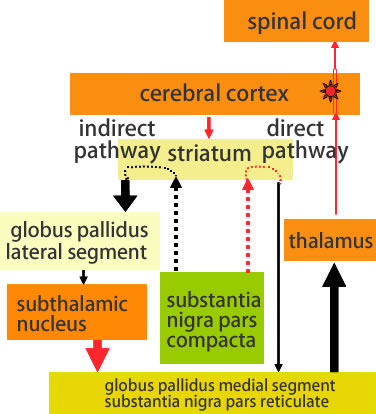
�yCerebral Cortex - Basal Ganglia Loop�z
 |
|
| Black�Finhibitory�@ |
�@Red�Fexcitatory |
| Bald arrow�Fhyperactivity �@ |
�@Narrow arrow�Fhypoactivity |
|
|
| �@substantia nigra pars compacta |
Produces dopamine which functions as a driving force for bodily movements |
| �� |
| �@striatum |
One of the basal ganglia. Control center for bodily movements. Needs dopamine to function well. |
| �� |
| �@direct/indirect pathways |
Sends inhibitory signals to the thalamus via cerebral basal ganglia (globus pallidus medial segment - subthalamic nucleus - globus pallidus medial segment/substantia nigra pars reticulate) |
| �� |
| �@thalamus |
Transmits signals from the striatum to the cerebral cortex. |
| �� |
| �@cerebral cortex |
Transmits signals from the thalamus to the spinal cord. |
| �� |
| �@spinal cord |
Transmits signals from the cerebral cortex to each muscle |
| �� |
| �@muscle |
Moves the body by contracting according to the signals from the nerves. |
|
�Q.Main Symptoms
- �yShaking (Tremor)�z�FRelatively slow tremor at rest - movement resembles rolling a pill on fingertips. Often starts in either right or left hand or leg.
- �yMuscle stiffness (rigidity)�z�FMuscles become rigid making it difficult to move smoothly. Bending and extending arms and legs are difficult and when someone else tries to assist in moving the limbs, there is a resistance that feels �gjerky.�h Difficulty turning the neck.
- �ySlowness of movement (Akinesia/Bradykinesia)�z�FDecreased movements. All movements become slow. Difficulty moving the legs forward and walking. Lack of facial expressions, voice becomes quiet and monotonous.
- �yPostural reflex disorder�z�FReflex that prevents one from falling when loss of balance is obstructed. Falling easily, even from a slight push. Inability to stop a fall, even when intending to.
�R.When to Choose DBS Surgery
- �yWhen side effects force one to reduce medication�z
�@�@�@��By stimulating the subthalamic nucleus, symptoms improve and the patient is able to reduce the dosage of oral medication.
- �yWhen everyday life becomes extremely difficult�z
�@�@�@��By improving symptoms during the �goff�h period (period when a medication�fs effect wears off and symptoms increase), the quality of life improves.
- �yWhen �gwearing off�h phenomenon or on/on-off effect becomes prominent�z
�@�@�@��When there is a large fluctuation in the symptoms and difficulty in controlling them with oral medication, DBS can reduce the �goff�h symptoms and maintain a well-controlled period.
�@�@�@���gWearing off�h is a phenomenon where symptoms manifest as the medication effect wears off over time.
�@�@�@�@ times when the medication effect appears or disappears regardless of the time of oral medication administration.
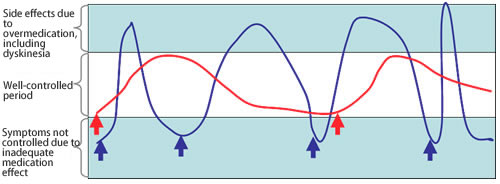
�S.Expected Outcome from Surgery
|
 |
|
 Difficulty controlling with oral medication Difficulty controlling with oral medication |
There is a large fluctuation of symptoms with oral medication, and the dyskinesia and �goff�h period last for a long time |
|
 Post-DBS Post-DBS |
After starting the stimulation, the dosage of oral medication is reduced, dyskinesia disappears, and the worsening of symptoms during �goff�h period disappears due to �gbottom-lifting effect,�h and the patient is able to maintain a mostly well-controlled state.
|
|
�T.Complications from surgery and side-effects of DBS
Concerning the rate of complications, while safety and efficacy of the surgery have been established, complications can occur in 1-2% of the cases.
|
- �yCerebral Hemorrhage�z�FIf the hemorrhage is large, there could be subsequent complications.
- �yInfection�z�FLocalized infection could occur around the implanted foreign objects.
�@�@�@�@�@�@If the infection is not well controlled using antibiotics, it may become necessary to remove the implanted electrodes, etc.
- �yBreakage�z�FIf there is a hardware breakage, surgery may be necessary to replace the component.
As for side effects, the patient may experience psychiatric symptoms including hallucinations or worsening of symptoms including temporary dyskinesia.
In many cases, these problems can be alleviated by reprogramming the pulse generator.
|
��Essential Tremor
1.What is Essential Tremor
- Essential tremor is an involuntary tremor that occurs in any part of the body, but often in hands.
- Tremor is induced when trying to hold the hand in the air. It also often occurs when one is actively moving.
(Graphospasm: becomes apparent in hand writing) - Family history cases often reflect increased susceptibility
- In many cases, symptoms increase when under mental stress
- Mild tremor is common (20 times more common than Parkinson�fs Disease), and is slower to progress
- Various medication treatments are available
�Q.Diagnosis of Essential Tremor
| Requirements |
| Bilaterality |
| Postural or action tremor ranging from the forearms to the hands |
| Tremor is continuous and can be visually confirmed |
| Exclusions |
| Other neurological manifestations |
| High probability that the tremor is psychogenic based on medical history or clinical manifestation |
| Sudden onset tremor or tremor that rapidly progresses |
| Orthostatic tremor that occurs in the lower limbs when standing |
| Tremor limited to vocalization, tongue and jaw, or lower limbs |
�R.Treatment Options for Essential Tremor
- �yMedications�z
�@�@�@��Beta-blocker including propranolol
�@�@�@�@�@Variety of antiepileptic agents including Mysoline
�@�@�@�@�@Antianxiety agents including benzodiazepine
- �yLifestyle changes�z
�@�@�@��Reduce consumption of caffeine, and increase relaxation
- �yLocal administration of botulinum�z
- �ySurgery�z
�@�@�@��If the tremor is severe and cannot be adequately controlled through various lifestyle changes and medications, and the patient has difficulty functioning in everyday life, surgery (deep brain stimulation in the thalamus) is indicated.
�S.DBS for Essential Tremor
- Advantages and disadvantages of stimulation therapy over thalamotomy
�@�@�@�@Advantage: 1) Less invasive, reversible, and can be performed bilaterally 2) Adjustable Disadvantage: Pulse generator is implanted under the skin + batteries need to be changed
- The VIM thalamus nucleus is targeted for stimulation. Tremor often reduces immediately after the stimulation begins.
- Given that essential tremor is generally slower to progress compared to Parkinson�fs Disease, long-term positive outcome of the stimulation therapy can be expected.
- Other than side effects that accompany general stimulation therapy, dysesthesia and articulation disorders can occur, but they can be reduced through adjustments.
- Mild tremor is more common (20 times more common than Parkinson�fs Disease), and is slower to progress.
 |
|
| Physicians on staff |
|
| Fumio Suzuki, M.D., Ph.D. |
|
�P�X�W�Q |
|
Department of Neurosurgery, Shiga University of Medical Science |
|
�P�X�W�X |
|
Department of Neurosurgery, Rakusai Shimizu Hospital |
|
�P�X�X�P |
|
Department of Neurosurgery, Shiga University of Medical Science |
|
�P�X�X�Q |
|
Studied at Hopital Henri-Mondor (France) |
|
�P�X�X�S |
|
Department of Neurosurgery, Shiga University of Medical Science |
|
�P�X�X�X |
|
Professor, Universite de Strasbourg |
|
�Q�O�O�S |
|
Kalorinska University (Sweden) |
|
�Q�O�P�O |
|
Department of Neurosurgery, Kotoh Kinen Hospital |
|
|
| Hisao Hirai, M.D., Ph.D. |
|
�P�X�X�P |
|
Department of Neurosurgery, Shiga University of Medical Science |
|
�P�X�X�Q |
|
Department of Neurosurgery, Nagahama Red Cross Hospital |
|
�P�X�X�T |
|
Department of Neurosurgery, Rakusai Shimizu Hospital |
|
�P�X�X�X |
|
Department of Neurosurgery, Hino Kinen Hospital |
|
�Q�O�O�P |
|
Department of Neurosurgery, Kotoh Kinen Hospital |
|
�Q�O�O�S |
|
Trained at Kalorinska University (Sweden) |
|
|
��UP |
|
|